
The Black/African American Healthcare Experience: Where Disparities Persist and Why It Matters
Filed Under: Market Research, Black / African American, Multicultural, CPG, Health Insurance

Ashleigh Williams
Senior Director, In-Person Qualitative Research

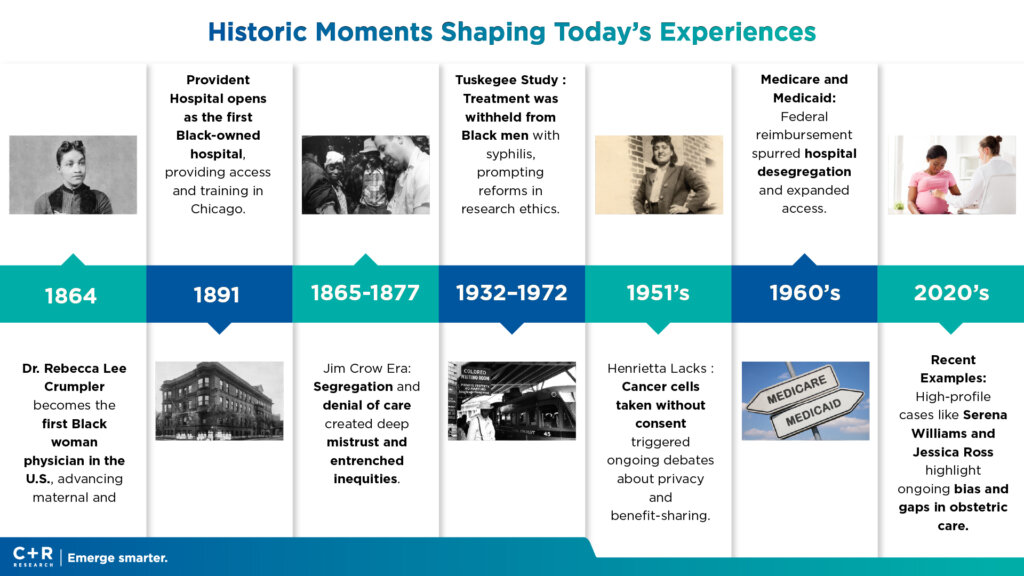
This month, we’re partnering across C+R’s Multicultural and Healthcare specialties to spotlight an issue drawing intensified national attention: healthcare experiences in the Black/African American community. From rising premiums and coverage churn to widely shared patient stories—like recent incidents where Mercedes Wells and Kiara Jones, Black mothers in active labor, were delayed or turned away, resulting in dangerous births outside of proper care —these are not isolated events or “new” phenomena. They’re the latest chapters in a long, intergenerational history of mistrust, unequal treatment, and structural barriers that continue to shape how Black/AA consumers engage with the U.S. health system today.
These stories circulate in families—from grandmother to mother to daughter—and inform behaviors: how appointments are scheduled (or avoided), where care is sought (or substituted), and which products are chosen to manage health and wellness at home. To kick off this story, we want to ground you in this journey of understanding with some overarching insights and statistics that give you a detailed picture of what Black/African Americans experience daily as they navigate healthcare spaces.
The Evidence: Where Disparities Show Up—and Why They Persist
1) Access to Coverage and Care
Black Americans remain more likely to be uninsured, and more likely to delay or forgo care due to cost. In 2023, 9.7% of Black people under 65 were uninsured vs. 6.5% of White people; despite ACA-era gains, gaps persist—especially in no expansion states where eligibility and affordability barriers remain high. Affordability pressure is rising: only 51% of Americans can access and afford quality care, with Black adults more likely to be “cost desperate,” unable to pay for needed care or medicines. These access constraints have downstream effects on preventive services and continuity of care.[kff.org], [aspe.hhs.gov] [ons.org]
2) Quality of Care and Patient Safety
Disparities are not just about coverage; they’re about care quality once inside the system. Federal assessments show Black patients receive worse care on more than half of measured indicators, with pronounced gaps in heart disease, cancer, stroke, maternal health, pain management, and surgical care—reflecting both structural factors (care deserts, facility resources) and interpersonal discrimination/microaggressions during clinical encounters. [nationalac…demies.org], [content.naic.org]. Black patients have a story that they either experienced primarily or secondarily that shapes the level of skepticism they have with healthcare and what care they are willing or unwilling to receive.
3) Health Status and Life Expectancy
The life expectancy gap remains wide. Black Americans’ life expectancy is ~74.0 years vs. 78.4 years nationally; Black men face even larger deficits. Self-rated health is poorer, with higher reports of fair/poor health—patterns that persisted through the pandemic recovery. [theglobals…istics.com]
Infant mortality is nearly double the national average (10.93 vs. 5.6 per 1,000 live births), signaling cumulative social and clinical inequities even before and just after birth. [cdc.gov]
4) Maternal Health: A Stark and Urgent Divide
In 2023, Black women died from pregnancy-related causes at 50.3 per 100,000 births, versus 14.5 for White, 12.4 for Hispanic, and 10.7 for Asian women—nearly 3.5× higher than White women. While the overall maternal mortality rate fell below pandemic peaks, the racial gap widened—underscoring systemic failures in access, bias recognition, and timely intervention. Notably, over 80% of pregnancy-related deaths are preventable. Recently publicized stories of Black mothers denied or delayed care highlight how interpersonal dismissal compounds risk in critical moments. [cdc.gov], [pbs.org], [sfgate.com] [detroitnews.com]. Stay tuned as we dig deeper into maternal health in the coming weeks of Black History Month.
5) Chronic Disease Burden
Black adults shoulder disproportionate burdens of hypertension (56.8% men; 61.0% women), obesity (55.9% women; 38.7% men), and diabetes—24% higher likelihood of diagnosis than the general population. These conditions multiply the risk for cardiovascular events, cancer progression, pregnancy complications, and COVID-related morbidity. [cdc.gov], [theglobals…istics.com]
6) Cancer and HIV Outcomes
Across many cancer types, Black patients exhibit lower survival—even after accounting for stage and income—due to later diagnoses, care quality differences, and structural barriers to guideline concordant treatment. National data show higher cancer death rates and consistently lower 5-year survival relative to White patients; importantly, survival gaps shrink when care processes are redesigned to ensure equitable, guideline-based therapy and barrier removal (transportation, navigation, cost support). Black people account for 43% of HIV deaths among those diagnosed and are less likely to be linked to, retained in, and suppressed by treatment—a treatment access and continuity problem more than a biological indicator. [kff.org] [cdc.gov]
7) Mistrust and Lived Experience
We wanted to dig into the intricacies of the relationship with healthcare and Black community by interviewing experts who experience these realities firsthand. We interviewed Jennifer who works as a therapist (clinical assessor/clinician) during the day and also serves as a professor teaching in social work programs. Specifically, she teaches full-time in the evening at Chicago State University in their social work master’s program and works as an adjunct professor for an MSW program in Aurora, IL.
The core issue Jennifer identifies based on her experience working with patients is that Black and Brown communities routinely feel dismissed, mistrusted, and unseen in healthcare settings. She describes this experience as leaving patients feeling “shame, disappointed, feeling unseen.”
Concrete examples of this bias showing up in their care include:
- Pain Minimization: Patients’ physical and mental health symptoms are downplayed or dismissed
- Eating Disorder Oversight: Symptoms in Black and Brown patients are overlooked
- Communication Patterns: Clinicians direct questions to companions instead of directly to patients
- Systemic Resource Withdrawal: Underserved neighborhoods lose access to healthcare resources, creating access gaps
History and contemporary encounters matter. A majority of Black adults (55%) report at least one negative interaction with providers (e.g., pain dismissed), and 51% believe the health care system was designed to hold Black people back. These perceptions are rooted in both historical abuses and ongoing clinical bias—and they shape care seeking strategies, including reliance on trusted community institutions and home based self management with OTC products and culturally trusted brands. [pewresearch.org], [pewresearch.org]
To overcome this bias, Jennifer employs multiple advocacy strategies:
- Patient Empowerment: Educating and role-playing with patients to help them learn how to advocate for themselves in medical visits.
- Direct Intervention: Accompanying patients and challenging clinicians when necessary.
- Policy Work: Writing letters and supporting bills to address systemic barriers.
This blog opens a month-long series examining health and care within the Black/African American community. Throughout February, we’ll share additional perspectives focused on mental health, overall wellness, and maternity care—each informed by historical context, present-day conditions, and the lived experiences that continue to shape how care is sought, delivered, and trusted.
The series will also consider the implications for organizations working in and around healthcare and consumer wellness. By exploring where barriers persist and where support can make a meaningful difference, the insights ahead aim to help your brand engage with greater awareness, cultural understanding, and responsibility.
We invite you to return throughout the month as the series unfolds, offering perspectives that connect history, health, and the evolving expectations placed on brands today.
